Spondylolisthesis is a condition in which one of the vertebrae in the spine slips forward in relation to the bone below it. Normally, vertebra align on top of one another, and their position is maintained by the discs, facet joints, and ligaments. Spondylolisthesis is mostly caused by the aging process, due to weakening joints and ligaments that hold the spine in the correct position. If the discs or facet joints become unstable due to wear and tear the vertebrae can slip. This in turn leads to arthritis of the joint, causing back pain. If the vertebra slips too much, it may press on a nerve, causing pain. Spondylolisthesis is the most common cause of back pain during teenage years and symptoms often occur during the teenage growth spurt. Degenerative spondylolisthesis occurs mostly after 40 years of age. There are six different types of spondylolisthesis, the most common being degenerative and isthmic.
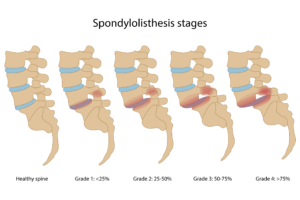
The forward slip of a vertebra decreases the stability of the spine.Spondylolisthesis varies in severity and is graded by the degree of forward slippage seen on imaging such as x-ray, CT or MRI.
- Grade I: 1% to 25% slip
- Grade II: 26% to 50% slip
- Grade III: 51% to 75% slip
- Grade IV: >75% slip
Symptoms
It is possible to have spondylolisthesis and experience no symptoms at all, however, the most common symptom is low back pain. It is often described as a tightness or stiffness that spreads across the lower back, similar to a muscle strain. Muscle spasms in the back of the thighs (hamstrings) can occur causing gait issues and changes in posture.
If the slipped vertebra is pressing on a nerve, patients may experience shooting back pains and radiating pain down the leg into the foot. It is not uncommon to experience tingling, numbness and weakness in the affected leg. As spondylolisthesis causes instability, symptoms may often worsen with increased activity or weight-bearing.
Causes
Spondylolisthesis in children or teenagers is usually caused by a birth defect or traumatic injury. In adults, the most common cause of spondylolisthesis is degeneration from natural wear and tear due to aging and arthritis.
The various types of spondylolisthesis include:
Congenital – birth defect causing abnormal bone formation resulting in slippage.
Isthmic-occurs as the result of spondylolysis, a condition that leads to small stress fractures in the vertebrae. In some cases, these fractures weaken the bone so much that it slips out of place. The condition can be triggered by certain sports that put a great deal of stress on the back, such as football, gymnastics, and weight lifting.
Degenerative – most common form. Occurs when the natural wear and tear due to aging and arthritis causes a vertebra to slip out of place. This form of spondylolisthesis usually occurs in people over 40.
Traumatic – occurs when an acute, traumatic injury leads to a spinal fracture or slippage.
Pathological – occurs when a tumour, disease or infection weakens the vertebrae, resulting in slippage.
Post-surgical – slippage that occurs or becomes worse after spinal surgery.
Diagnosis
Spondylolisthesis is diagnosed using a combination of physical examination, medical history and X-rays or other imaging.
Spondylolysis and spondylolisthesis can be diagnosed through the use of X-rays, CT or MRI scan. In most cases, the degree of slippage is easily measured using regular X-rays. An MRI is often used to better visualise the degree of compression of the spinal cord or nerves. A CT can be used to better visualise the bones.
Treatment
Treatment for spondylolisthesis depends on several factors:
- Extent of the slip
- Severity of the symptoms.
- Age of person
- Overall health of the person,
Treatment almost always begins with conservative management and only progresses to surgery when all other treatment options have failed.
Medications: Anti-inflammatory medications (NSAIDS) may be used for short periods to help control pain and ease muscle spasms. Short periods of bed rest may help with acute painful episodes. Stronger medications might be prescribed if NSAIDs do not provide relief.
Rest: Taking a break from activities or sports that exacerbate pain is recommended where possible. Short periods of bed rest may help with acute painful episodes
Steroid injections— These are an option for more severe cases. The aim is to reduce inflammation and reduce pain by injecting medication directly in the space surrounding the spine.
Physiotherapy: Exercises are aimed at improving core stability. These exercises strengthen the abdominal and/or back muscles. Strengthening the back muscles can reduce the mechanical symptoms resulting from the segmental instability.
Surgery: Surgery may be required if the vertebra continues to slip or if the pain is not relieved by conservative treatment. The goal of surgery is to relieve the pain associated with an irritated nerve and to stabilise the spine where the vertebra has slipped. Surgery must address the mechanical symptoms and the compressive symptoms if they are present. The nerves exiting the spine must be decompressed to alleviate pain and neurological dysfunction. This will usually require a spinal fusion.